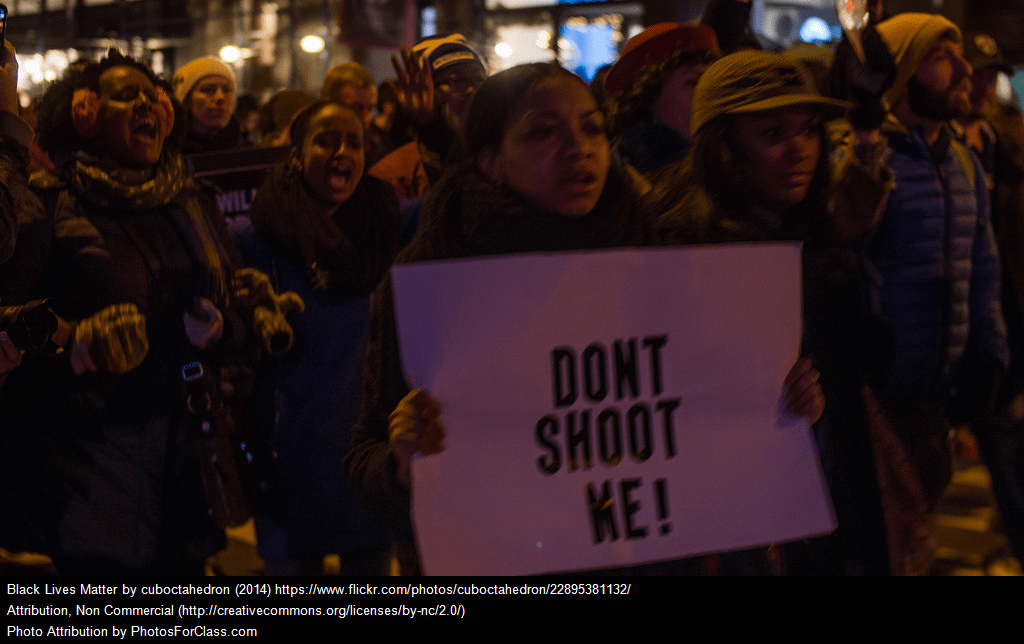
Our country is facing a national identity crisis. In only one week, we have seen our country divided in ways that many of us have never seen. At this historical crossroad, we are questioning who we are as a country and the values that make our country exceptional. One of those values is our belief that all men are created equal, regardless of their ethnicity or religion.
Executive orders signed by President Donald Trump during his first week in the White House call into question our value of equality. These orders severely target immigrants living and working in our neighborhoods and refugees fleeing persecution and war.
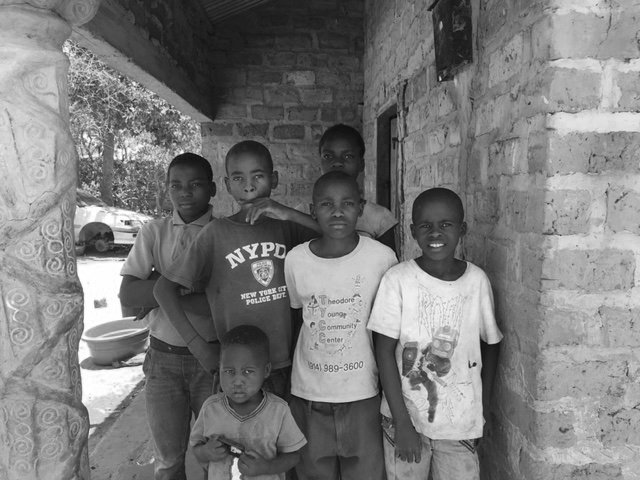
The Daniel Society stands with immigrants and refugees. We welcome immigrants and choose to love our neighbors. Our neighbors are immigrants and we are immigrants.

(Photo credit: Genna Martin / seattlepi.com/AP)
Over the coming months, The Daniel Society’s Center for Law and Justice will take steps to support immigrants and refugees, including:
-
Providing free neighborhood-based immigration legal services to low-income immigrants
-
Expanding our Central America Asylum Project to represent more children who fled persecution in Central America
-
Hosting community workshops that educate immigrants about their Constitutional rights
-
Facilitating roundtable “talks” with immigrants to create action plans for policymakers
However, we cannot do this work alone. We urge you to get involved with us or other organizations that are working to strengthen immigrant communities. Let’s send a message that America still is, and always will be, a welcoming country.
Download our statement here. To learn more about our work and progress, visit us at http://www.danielsociety.org/law-justice-initiatives.